Tuberculous mastitis (TM) is a rare chronic granulomatous disease predominantly caused by Mycobacterium tuberculosis.1 TM accounts for less than 0.1% of all breast diseases worldwide, whereas it is more common in endemic regions (3–4.5%).2,3 TM is more prevalent in the reproductive age group, especially during the lactation period, when patients are more susceptible since the lactating breast is more vascular and predisposed to trauma.4 It can mimic other breast conditions, such as carcinoma or pyogenic abscesses, sarcoidosis, fungal infections and other granulomatous diseases, leading to misdiagnosis.4,5
Clinically, it has variable presentations, from focal or diffuse alterations like solitary or multiple breast masses, abscesses, sinus tracts, skin ulcers, nipple retraction, peau d’orange and breast oedema.1,6 The most common presentation is a solitary breast lump, often located in the upper outer quadrant, with or without constitutional symptoms.2,6 Tewari and Shukla divided TM into nodular, disseminated and abscess.1,7
Diagnosis remains challenging due to the paucibacillary nature of the disease.1 Conventional methods include acid-fast bacilli (AFB) culture, GeneXpert and smear on Ziehl–Neelsen (ZN) stain. AFB smear often lacks sensitivity, while culturing can be costly.8 Polymerase chain reaction (PCR) and fine-needle aspiration cytology (FNAC) are used infrequently in low- and middle-income countries (LMICs) due to limited laboratory infrastructure and cost constraints.9 Histopathological examination provides a more definitive diagnosis by identifying chronic granulomatous inflammation, caseous necrosis and Langhans-type giant cells.9 Imaging modalities like chest X-ray, mammography, breast ultrasound, chest Computed tomography (CT) scan and Magnetic Resonance Imaging (MRI) help characterize the lesion further.8 For example, CT is useful for evaluating lesions with deep retromammary localization and thoracic wall involvement.2 MRI is also a useful modality for showing the extension of the fistula tract into deep tissues, but does not give a conclusive diagnosis and, once again, is not widely available in LMICs.2,9 In patients from endemic areas, tuberculosis infection should be suspected in cases of recurrent mastitis refractory to antibiotic treatment.10
Treatment typically involves anti-tuberculosis medications, with surgical intervention, such as drainage or excision, reserved for resistant or extensive cases.7 A common regimen includes an initial intensive 2-month phase with isoniazid, rifampicin, pyrazinamide and ethambutol, followed by a 4-month continuation phase with isoniazid and rifampicin for drug-susceptible Tuberculosis (TB), which can be extended to 12 months or up to 18 months based on clinical response.2,8
This retrospective study evaluates 25 patients with TM for diagnostic challenges in an endemic area in an LMIC setup, stressing the need for high clinical suspicion and multidisciplinary approaches for accurate diagnosis and effective management.
Materials and methods
Study design and setting
This was a retrospective case series conducted from May 2012 to May 2025 in the Department of General Surgery and the Department of Infectious Disease, at the Indus Hospital, Karachi.
Demographic Data:
Age, Gender (all females), presenting complaint, duration of symptoms, lactation or pregnancy history, past history of TB, history of concomitant TB, any skin changes (retraction, nipple inversion or ulceration), imaging findings (ultrasound, Birads score), biopsy, HIV status, anti tuberculous drugs and their duration, treatment outcome and interventions included.
Source population and selection criteria
A total of 220 patients from hospital records who presented in out-patient clinics with breast diseases were screened, and patients were selected if they had definitive, probable or possible TB mastitis. Patients who did not show a response to treatment were excluded from the study.
Case definitions
Definitive TM: when proven by microbiological testing, such as GeneXpert, AFB smear and AFB culture, or by histopathology (taken via Tru-cut biopsy technique) with the presence of chronic granulomatous inflammation and caseating granulomas.
Probable TM: when non-caseating granulomatous mastitis or histiocytes were present with clinico-radiological evidence and epidemiological risk.
Possible TM was considered when the patient had negative TB tests, clinically no response to broad-spectrum antibiotics and a response to a full course of anti-tuberculous therapy (ATT).
Response to treatment was considered when there was resolution of a lump, abscess, healing of sinus tracts, weight gain, improvement in appetite, remission of fever or resolution of radiological findings.11 If patients had partial resolution of symptoms, they were labelled as improved.
Demographic data
Clinical data collected: demographic data (Age, Gender), symptoms, duration, lactation or pregnancy history, past history of TB, history of concomitant TB, any skin changes (retraction, nipple inversion or ulceration), ultrasound imaging [Breast Imaging-Reporting and Data System (BIRADS)], treatment and outcome.
Laboratory methods: microbiology, GeneXpert, AFB culture, AFB smear, ZN stain, HIV status and biopsy (taken via trucut/FNAC).
Ethical approval
The study was approved by the Institutional Review Board (IRB) administration of Indus Hospital and Health Network (IHHN) (study number: IHHN_IRB_2025_02_014; date of approval: 21 February 2025). The IRB waived the requirement for informed consent due to the retrospective nature of the study and the anonymized data analysis.
Statistical analysis
IBM SPSS Statistics version 26, released in 2018 was used for statistical descriptive analysis. Categorical variables were expressed as frequencies and percentages. Normally distributed continuous variables were presented as means and standard deviations.
Results
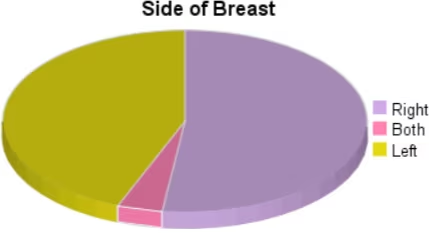
The study population included 25 females, ranging in age from 20 to 65, with a mean age of 37.2 ± 8.3 years. Three out of 25 (12%) were lactating, and another 3/25 (12%) were pregnant when presented. Single breast involvement was present in 24/25 patients (96%), and 1/25 case (4%) had both breasts involvement (Figure 1).
Figure 1: Side of the breast involved
Clinical presentation
Clinical examination was focused on the presence or absence of a breast mass, with or without abscess, sinus tracts development, lesion location and associated skin changes like peau d’orange or nipple retraction. The most common clinical presentation was a breast lump, observed in 13/25 patients (52%), followed by a lump with abscess in 10/25 patients (40%), most frequently located in the central region in 8/25 cases (32%). The second most common site was the upper outer quadrant, seen in 6/25 patients (24%); others had variable locations. Around 9/25 patients (36%) developed single or multiple sinus tracts associated with abscess. Skin ulceration was reported in 1/25 patients (4%). Four out of 25 patients (16%) had nipple retraction, while two of them also had peau d’orange (8%), and a single patient (4%) had nipple inversion. Twenty-one out of 25 patients (84%) had an acute onset of symptoms with a duration of less than 6 months, with most patients, 8/25 (32%), presenting before or around 1 month, while 4/25 patients (16%) had a duration of more than 6 months (Figure 2). All cases failed to respond to an initial course of empirical broad-spectrum antibiotics. A single patient had a history of relapse. Two out of 25 patients (8%) had disseminated TB, with one case each of pulmonary tuberculosis and tuberculous adenitis of cervical lymph nodes. One out of 25 patients (4%) had a history of psoas abscess due to extrapulmonary tuberculosis. Four out of 25 patients (16%) had a history of tuberculosis contact positivity (Table 1).
Figure 2: Duration of symptoms among patients
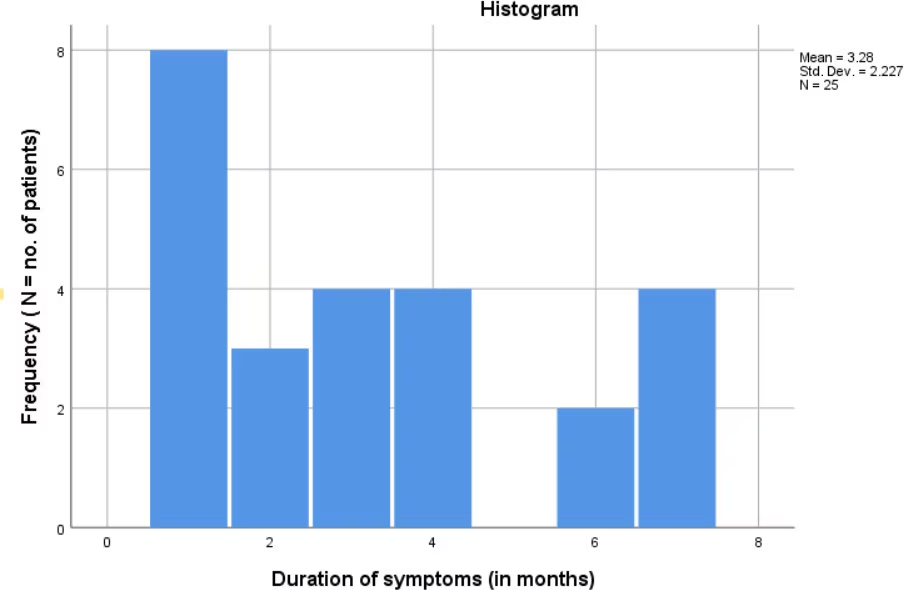
Std. Dev. = standard deviation.
Table 1: Clinical presentation
| Clinical features | n (%) |
| Lumps | 13 (52%) |
| Lumps with abscess | 10 (40%) |
| Abscess | 2 (8%) |
| Single sinus tract | 6 (24%) |
| Multiple sinus tracts | 3 (12%) |
| Ulceration | 1 (4%) |
| Relapse | 1 (4%) |
| Nipple retraction | 4 (16%) |
| Nipple inversion | 1 (4%) |
| Peau d’orange | 2 (8%) |
| Disseminated | |
| Pulmonary Tuberculosis | 1 (4%) |
| Cervical TB adenitis | 1 (4%) |
| Past history | |
| Psoas TB abscess | 1 (4%) |
| TB contact | 4 (16%) |
Radiographical findings
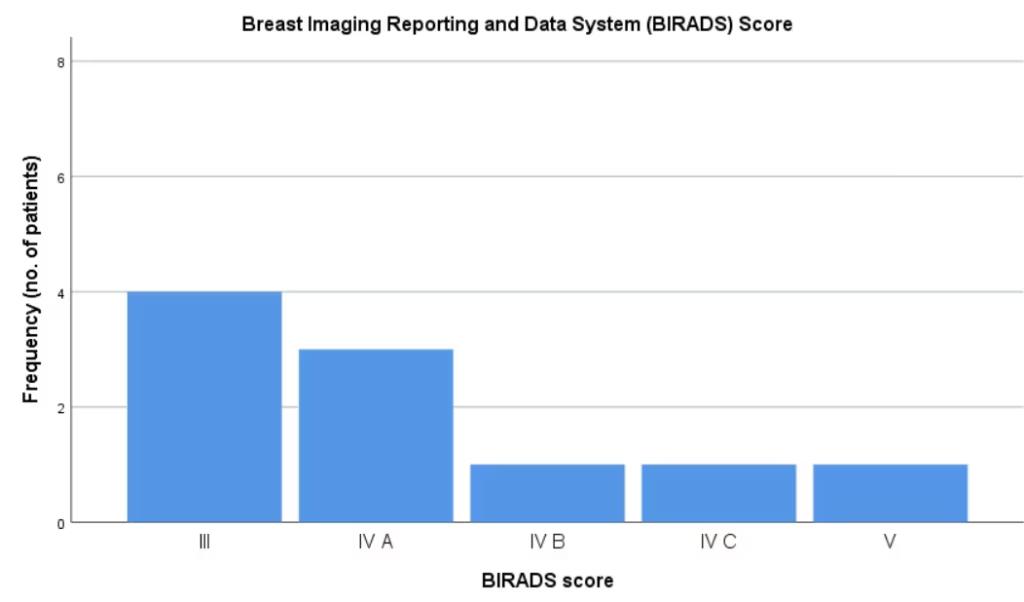
Ultrasound breast findings and BIRADS scores were evaluated. It showed that 10/25 patients (40%) had hypoechoic lesions, and the other 10/25 patients (40%) had internal echoes with collections, whereas 5/25 patients (20%) had both hypoechoic lesions and internal echoes with collections (Table 2). Ten out of 25 patients (40%) had single collections with internal echoes, 7/25 (28%) had multiple collections with internal echoes, and 1/25 (4%) had multiple intercommunicating collections. Eight out of 20 patients (40%) had a BIRADS score of II, and 4/20 patients (20%) had a BIRADS score of III (Figure 3). Three out of 20 patients (15%) had BIRADS score of IV A, whereas there were cases of each BIRADS IV B, IV C (Figure 4) and V, which are 5% each; collectively, 6/20 patients (30%) had a high BIRADS score suspicious for malignancy (Figure 5). Two out of 20 patients (10%) had BIRADS I, whereas 5/25 patients (20%) had ultrasounds done at an outside facility which did not comment on BIRADS.
Table 2: Radiological/laboratory findings
| Radiological/laboratory findings | |
| Characteristics | No. of positive/tested (%) |
| Hypoechoic | 10/25 (40%) |
| Internal echoes | 10/25 (40%) |
| Hypoechoic with internal echoes | 5/25 (20%) |
| Features | |
| Granulomas | 16/24 (66.7%) |
| Histiocytes | 5/24 (20.8%) |
| Neutrophils | 3/24 (16%) |
| Test | |
| Biopsy | 21/24 (87.5%) |
| Culture | 2/8 (25%) |
| GeneXpert | 2/13 (15.4%) |
| Smear | 2/12 (16.7%) |
Figure 3: Ultrasound Imaging of breast- categorized as BIRADS score III showing
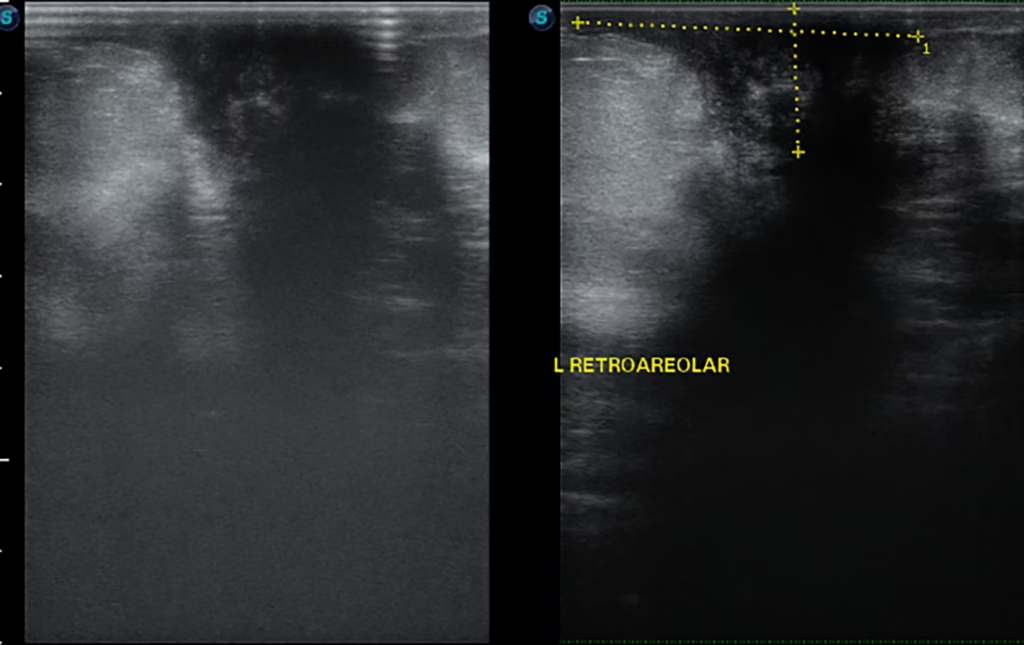
An irregular retroareolar collection is noted in the left breast subcutaneous tissue, measuring 3.7 × 1.5 cm
Figure 4: Ultrasound Imaging of breast -categorized as BIRADS score IV C showing
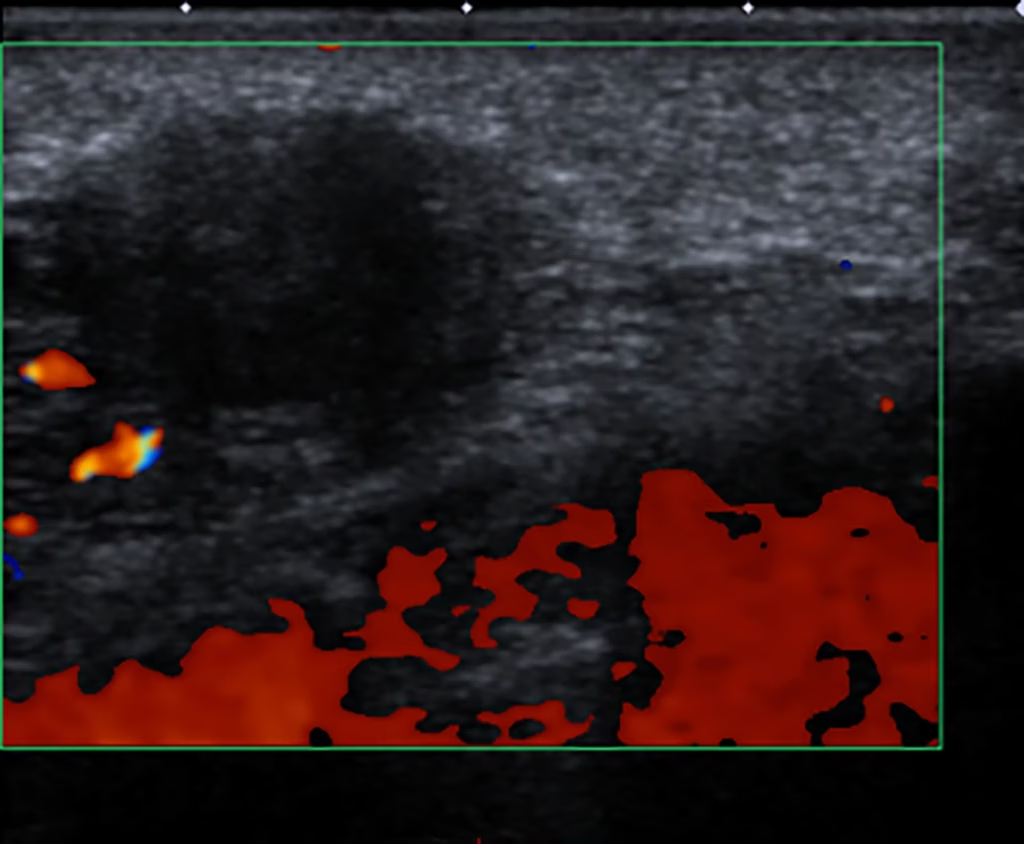
Ill-defined, heterogenously, highly vascular lump in the left breast
Figure 5: BIRADS score
Laboratory findings
Biopsies had the highest diagnostic yield, at 87.5%, with 16/24 patients (66.7%) having granulomas, 5/24 patients (20.8%) showing only histiocytes, and 3/24 patients (12.5%) having other non-TB findings, like neutrophilic aggregates (Table 2). One patient did not undergo a biopsy, as TB mastitis was already confirmed through microbiologic workup. However, this yield is still lower than that mentioned in a systematic review, which is 92.8%.1
The AFB culture diagnostic yield was 2/8 (25%), whereas 6/8 (75%) had negative results. GeneXpert showed 2/13 positives (15.4%), and 11/13 patients (84.6%) were negative. Among the 2 patients who were positive for microbiological tuberculous workup, 1 tested positive on the first sample, whereas the other tested positive after the second debridement. Two out of 12 patients had positive AFB smear (16.7%), while 10/12 (83.3%) had negative results (Table 2). HIV status was negative in 7/7 tested patients.
Management
Ten out of 25 patients (40%) got incision and drainage, among whom 4/25 (16%) got it done twice. Four out of 25 patients (16%) got excision of the lump done. The majority of patients, 7/25 (28%), were given treatment for 6 months, and 5/25 patients (20%) received treatment for 8 months; the rest had variable durations, as mentioned (Figure 6). Four out of 25 patients (16%) received ATT empirically based on high clinical suspicion due to chronicity or recurrence of symptoms despite all TB workup being negative, after exclusion of malignancy and serious bacterial infection. Fourteen out of 25 patients (56%) had a complete response to treatment, and 9/25 patients (36%) had improved, of which 3/25 (12%) had on-going treatment, and 2/25 patients (8%) were lost to follow-up (Table 3).
Figure 6: Duration of treatment
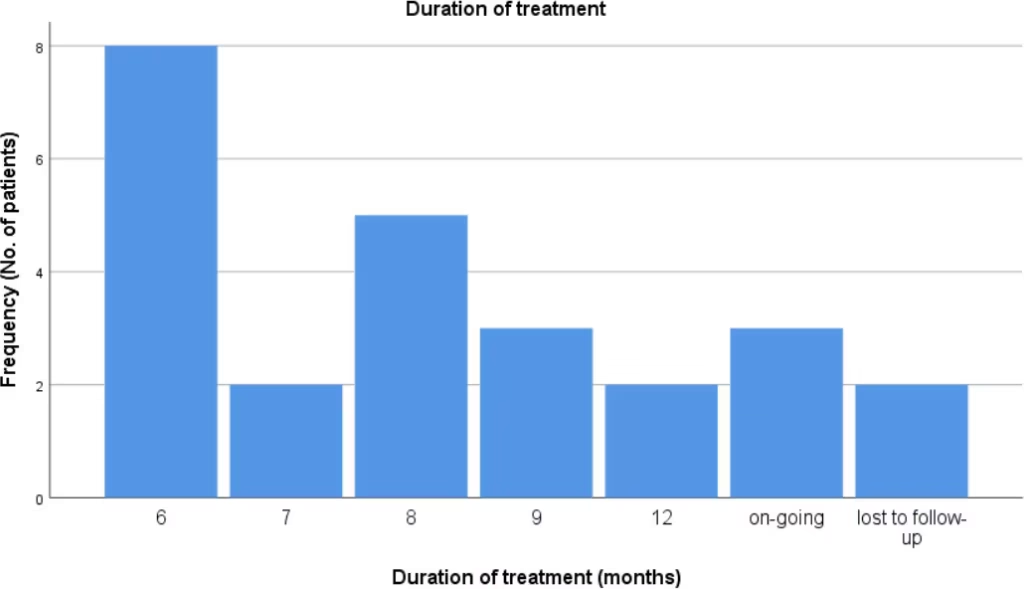
Table 3: Treatment outcome
| Outcome | n (%) |
| Treated | 14 (56%) |
| Improved | 9 (36%) |
| On-going | 3 (12%) |
| Lost to follow-up | 2 (8%) |
Discussion
TM is a rare disorder with diverse presentations, mimicking other benign and malignant lesions of the breast, leading to misdiagnosis. In endemic regions like India, the incidence of TM can be as high as 3–4.5%.2 A study in Pakistan showed an incidence of 1.2% of cases between 2018 and 2019.11
Clinical presentation
This study highlights the variable clinical presentations encountered, which often lead to misdiagnosis. As TM is common in women of reproductive age groups, our study shows that a total of 24% of the cases were either pregnant or lactating at the time of presentation (12% in each group), within the range of 7–33% as shown in previous studies.1 It is considered to be primary when the breast lesion is the only manifestation of tuberculosis, and secondary when there is a demonstrable focus of tuberculosis elsewhere in the body, as per the Mckeown and Wilkinson classification.12 The average duration of symptoms before diagnosis is highly variable, spanning from a few weeks in Europe to more than 7 months in India and sub-Saharan Africa.13 This includes both patient and health system delays and reflects the range of cultural, psychological and economic components, as well as the diagnostic challenges.13 However, in our study, 84% of patients had an acute duration of symptoms of less than 6 months, with most patients (32%) presenting around 1 month, while 16% of patients had a duration of more than 6 months. TM is rare in males, with only 3% of cases in another study, and bilateral involvement is also very uncommon (3%).1,8 In the present study, none of the patients were male, and bilateral presentation was seen in only 4% of patients. According to Wilson, the right and left sides of the breast were equally involved often. In contrast, Pal reported that there is a slight tendency for the right breast to be more frequently affected, as it was in our case series.14 The most frequent clinical finding in our study was a palpable lump, consistent with the literature, especially in the central area, in 32% of cases, followed by involvement of the upper outer quadrant (24%), consistent with the literature.1 The lumps were present in 52% of patients, followed by the presentation of both lump and abscesses in 40% of patients, while 74.9% of patients had lumps and 14.9% of patients had abscesses, as reported in a systematic review.9 Around 36% of the cases also exhibited sinus tract formation, either single or multiple, comparable to 29.4% in another study.1 One patient (4%) had developed skin ulceration. Other signs mimicking features of carcinoma included nipple retraction (16%), peau d’orange (8%) and nipple inversion (4%). These features are typical of TM, which often mimics both inflammatory and malignant breast conditions, making diagnosis particularly challenging. Additionally, some patients had concurrent pulmonary or extrapulmonary TB, including cervical lymphadenitis and psoas abscess in the past, which emphasizes the need to consider systemic disease when evaluating atypical breast lesions. Importantly, contact with a TB-positive individual was present in 16% of our patients, whereas this was 15.2% in another study.13
Laboratory diagnosis
The gold standard diagnosis of TM is by bacteriological culture of breast tissue. However, in TM, the bacilli are isolated in only 25% of cases, and AFB are identified in only 12% of patients.8 In our study, the diagnostic yield of GeneXpert was 15.4%, AFB smear 16.7% and AFB culture 25%. The low sensitivity of microbiological tests in our cohort underscores the fact that TM is often a paucibacillary disease. Consequently, histopathological demonstration of granulomas remains the diagnostic cornerstone in our setting, despite being an invasive procedure. The biopsy had the highest diagnostic yield of 87.5%, which is comparable to, though slightly lower than, the 92.8% yield reported in a systemic review.9 This signifies the importance of testing all patients with suspicious lesions, whether lumps or abscesses, for tuberculosis. Previous studies have shown that AFB staining is positive in 15.7% of patients.15 While our study had histopathological samples, Zeihl–Nelson staining was negative in all 24 patients. The advent of multidrug-resistant strains and HIV infection is steadily increasing its extrapulmonary manifestation in developing countries, predominantly among migrant population.16 However, we had tested the HIV status of seven patients, all of whom were negative. Our article highlights a gap in HIV testing in the initial years of our TB treatment programme. The current practice at our centre, as per national and international TB guidelines, is to screen all cases of TB for HIV at the time of initial evaluation. An alternative is PCR to identify M. tuberculosis genetic material, but it is rarely used in LMICs, as mentioned. FNAC detects the presence of epithelioid cell granulomas and necrosis, and is often used instead, but has drawbacks, as differential diagnosis is difficult in cases of granulomatous mastitis and sarcoidosis, for instance.9
Imaging study
Ultrasonography of the breast is cheap, easily accessible and helps characterize the lesion better (especially cystic from solid lesions) without radiation exposure.15 A significant number of patients (40%) had hypoechoic lesions, and another 40% had collections with internal echoes. A smaller group, 20%, showed both findings. While these sonographic features suggest an infective aetiology, they lack specificity and can sometimes resemble neoplastic changes. The BIRADS scores were high, IV or V, with suspicion for malignancy in 30% of the cases, as compared to 43.5% seen in another study.13 Multiple abscesses were seen in 28% of patients, and one patient exhibited intercommunicating collections, a classic but rare sign of disseminated TM. In contrast, another study reported 56.5% of cases with hypoechoic mass and 11% of cases with abscesses.13
Management and outcomes
The cornerstone of treatment remains antitubercular therapy, prescribed for a minimum of 6 months. To prevent recurrence, or when the clinical response is slow, a prolonged treatment duration has been reported, as was the case with our patients.5 Otherwise, most patients were managed with standard anti-TB therapy, typically for a duration of 6–8 months, consistent with global treatment recommendations. One patient had mono-drug-resistant TB, but she showed complete response with first-line ATT drugs. In contrast, another patient had all drug-susceptible TB on reports but only showed improvement after the addition of levofloxacin to the regimen. Notably, a significant proportion of patients (16%) with negative TB workup were successfully treated with empirical anti-TB therapy based on clinical judgement on recurrence of symptoms or abscesses not responding to broad-spectrum antibiotics, after taking the multidisciplinary team on-board. These diversities underline the importance of clinical acumen in cases where laboratory tests are inconclusive, and all other possible causes have been ruled out. Surgical intervention was necessary in over a third of the cases, primarily involving incision and drainage of abscesses in 40% of patients, where 16% of patients had needed it twice. A smaller number of patients (16%) underwent excision of the lesion.4 While the systematic review showed incision and drainage done in 23.1% of cases and excision of lumps done in 38.6% of cases.9
Encouragingly, treatment outcomes were largely positive. Overall, 56% of patients showed complete resolution, while 36% had notable clinical improvement, 12% of whom were still completing treatment at the time of follow-up. Eight per cent of patients were lost to follow-up. This response highlights the overall effectiveness of timely initiation of ATT, even when bacteriological confirmation is absent.
Limitations
This study on breast TM faces several limitations, including its retrospective nature, which can introduce biases and limit the ability to establish causality. The rarity of the disease often results in small sample sizes, reducing the generalizability of the findings. From our institutional records, approximately 10,092 cases of extrapulmonary tuberculosis were recorded between 2008 and 2024, of which 25 (0.25%) were TM. There is a possibility that all data on TB mastitis from our institution could not have been included due to the non-coding of old data, producing a bias. Also, due to belonging to an LMIC, we could not get all the TB testing done, such as PCR, so our diagnostic ability was limited and relied more on biopsies and our clinical practices. There was an inability to get the HIV status of all patients, which produces a bias. There is often a delay in diagnosing breast tuberculosis, complicating treatment and outcomes. There are no standard methods for monitoring clinical response; therefore, response was monitored in our study based on improvement in symptoms, localized, constitutional and radiological symptoms; however, we have not included the follow-up duration for our patients.
Conclusion
Our study focuses on the diverse presentations of TB mastitis, from a benign condition to a malignant appearance, along with the diagnostic challenges and variations in management according to clinical response. Our findings support the role of a multidisciplinary approach, and clinical judgement, which often guides management, especially when laboratory findings are non-conclusive. A high index of suspicion is warranted in endemic regions, especially in reproductive age groups, pregnant or lactating, presenting with acute-onset symptoms, as early treatment can lead to excellent outcomes and prevent complications such as chronic sinuses or unnecessary surgical procedures. Our study hypothesizes to get a tuberculosis workup along with biopsies in patients suspected of malignancies, and also to repeat the tuberculosis workup, especially in cases of underdiagnosed acute mastitis; a trial of anti-tuberculous drugs may be considered after exclusion of malignancy and serious bacterial infections, with close follow-up.