

Often mistaken for more common gynecological conditions, female genital schistosomiasis can remain undiagnosed for years. Dr Marc Steben explains the key clinical features clinicians should not miss.
 We spoke with Dr Marc Steben about female genital schistosomiasis (FGS), why it remains under-recognized in clinical practice and what clinicians should know when evaluating women with unexplained gynecological symptoms.
We spoke with Dr Marc Steben about female genital schistosomiasis (FGS), why it remains under-recognized in clinical practice and what clinicians should know when evaluating women with unexplained gynecological symptoms.
Dr Marc Steben is a Family Physician; Co-PI, Papillomavirus automated visual examination project at the National Cancer Institute; and Chair of the Education Committee at the International Papillomavirus Society, Montreal, Quebec, Canada.
“Many women see multiple healthcare providers before receiving a diagnosis. It is not uncommon for women to spend decades seeking answers before someone recognizes the condition.”

Could you briefly describe female genital schistosomiasis and explain why it is so frequently missed in clinical practice?
Female genital schistosomiasis (FGS) is an infection acquired through the skin following exposure to contaminated freshwater, predominantly in rural sub-Saharan Africa where freshwater sources are contaminated with the parasite, a manifestation mainly of Schistosoma haematobium infection. For reasons that are not fully understood, the parasite establishes itself in the vesical venous plexus. From there, it invades the bladder, which is why both men and women can present with hematuria.
In women, however, the parasite can also migrate to the genital tract. As a result, women may present with vaginal discharge, pain during intercourse, bleeding during intercourse and infertility if the uterus is involved. There is also an association with HIV acquisition, human papillomavirus (HPV) acquisition and HPV persistence. FGS it is not acquired by sex but partners are very likely to be infected in the same fresh water source.
We miss FGS because many clinicians assume it is a disease that remains confined to Africa. However, cases have already been identified in Europe, including Corsica. Infected individuals can contaminate freshwater sources through urination and defecation, and climate change may further influence transmission patterns.
Women with FGS often present with symptoms and seek medical care, but many healthcare professionals have never been trained to recognize the condition. Increasing migration means that clinicians in non-endemic countries are more likely to encounter affected patients.
These women frequently undergo extensive investigations, yet results often come back normal because appropriate schistosomiasis testing is not widely available. Serology is the most commonly available test, but it only indicates previous exposure and is therefore of limited diagnostic value. Newer diagnostic approaches, including nucleic acid amplification techniques (NAAT) and visual assessment supported by artificial intelligence, are being explored but are not yet widely available.
Importantly, we should not only think about migrants and refugees. Travelers who swim in freshwater during vacations may also develop FGS months later. The disease travels with people.
Which symptoms and patient characteristics should raise suspicion for FGS?
One important group is women living with HIV who come from endemic countries. We know there is a link between schistosomiasis and HIV acquisition.
Many affected women also come from regions where HPV vaccination and cervical screening programs are limited. If HIV, HPV and schistosomiasis occur together, it creates what I often call the “infernal trio” of the tropics.
Clinicians should consider FGS in women presenting with unexplained vaginal discharge. If microscopy demonstrates abundant white blood cells but testing for gonorrhea, chlamydia, Mycoplasma genitalium and trichomoniasis is negative, schistosomiasis should be considered.
Current World Health Organization (WHO) algorithms for female genital discharge do not mention FGS at all.
What are the biggest challenges in diagnosing FGS?
The biggest challenge is that most healthcare professionals have never been trained to recognize it.
Even in endemic countries, where schistosome infection is common, many clinicians report seeing only a small number of cases. The reality is that they have probably seen more cases than they realize.
The most obvious cases are difficult to miss because they present with classic findings. However, many women present with chronic pelvic pain, chronic vaginal discharge or other non-specific symptoms. These symptoms are rarely life-threatening, but they can persist for years and significantly affect quality of life.
I often tell clinicians: “You have probably seen FGS before; you just did not know what it was.”
Many women see multiple healthcare providers before receiving a diagnosis. It is not uncommon for women to spend decades seeking answers before someone recognizes the condition.
What practical advice would you give clinicians who suspect FGS?
These women benefit from seeing healthcare professionals who are familiar with tropical medicine and neglected tropical diseases. Knowledge is improving, but diagnostic testing remains a challenge. Many tests are not routinely available and samples may need to be sent to specialized referral laboratories.
Clinicians should also be aware of the characteristic colposcopic findings associated with FGS. The WHO Pocket Atlas for Female Genital Schistosomiasis contains excellent visual examples.
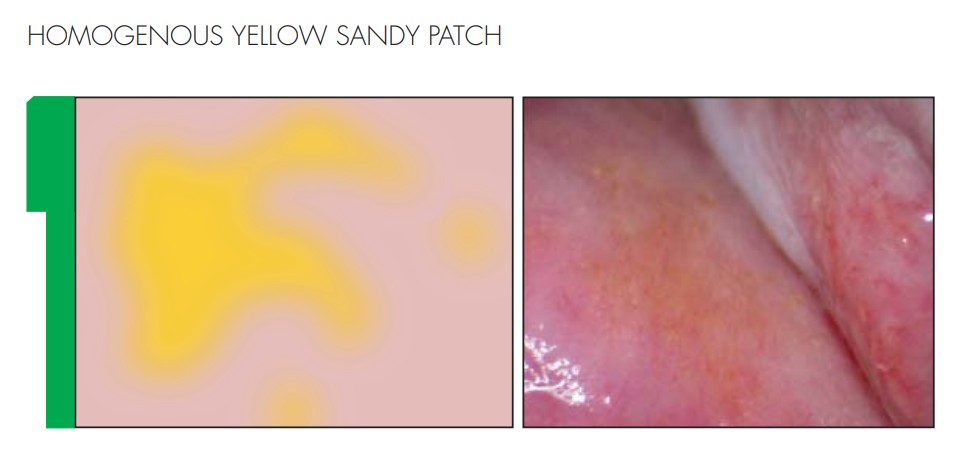
Colposcopic findings associated with FGS:
- One feature is the presence of grainy sandy patches that resemble small yellow grains of rice.
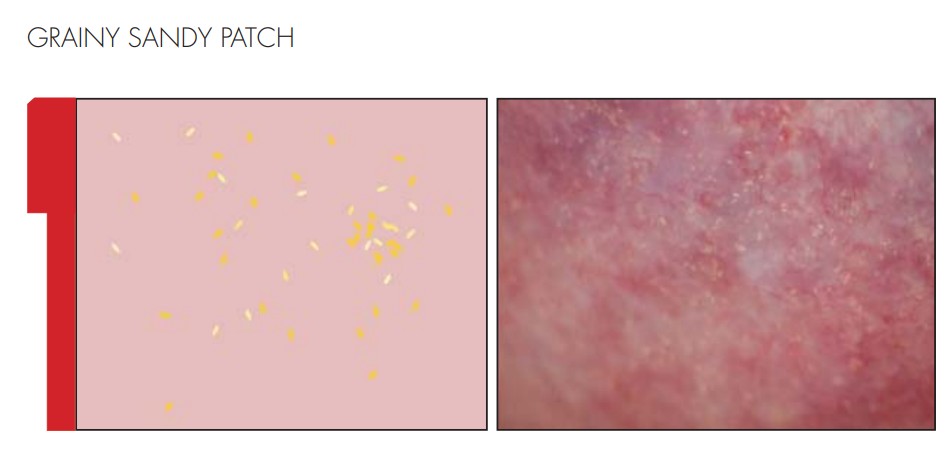
- Another is the presence of abnormal, irregularly branching blood vessels. These vessels appear disorganized and differ from normal vascular patterns.

- Another feature can be presence of homogeneous yellow sandy patches, which appear smooth, discolored areas of the cervical or vaginal mucosa.
- Some women also develop what are known as rubbery papules. These lesions can range from a few millimeters to a few centimeters in size. Unlike vesicular lesions associated with herpes infection, they feel firm and rubbery on examination.
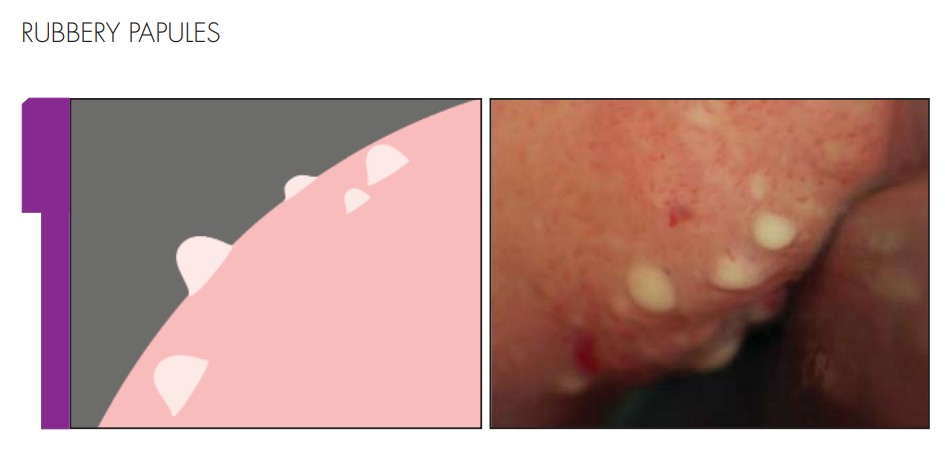
Images above have been reproduced with permission from: Female genital schistosomiasis: A pocket atlas for clinical health-care professionals. www.who.int/publications/i/item/9789241509299: World Health Organization; 2015. Licence: CC BY-NC-SA 3.0 IGO.
These visual findings can be highly suggestive of FGS and should prompt further investigation.
Traditional diagnostic approaches, including urine microscopy and serology, have limited sensitivity. Positive results can be helpful, but negative results do not exclude the diagnosis. 24 hours urine is of lower sensitivity than NAAT testing but is cumbersome but may be the only test available.
Is there anything else clinicians should know?
Praziquantel remains the key treatment for schistosomiasis and is widely used in preventive treatment campaigns in endemic countries, particularly among school-aged girls and, in some settings, boys as well.
Praziquantel dosage
- Adults and children 1 year of age and older: Dose is based on body weight and must be determined by your doctor.
- The dose is 20 milligrams (mg) per kilogram (kg) of body weight taken 3 times a day for 1 day only.
- Each dose should be at least 4 hours apart and not more than 6 hours apart.
For individuals with a history of repeated freshwater exposure in endemic areas, even in the absence of symptoms, pre-emptive treatment with praziquantel may be appropriate.
One emerging challenge in Europe is drug availability. Some countries no longer routinely maintain stocks of praziquantel. As a result, treatment may need to be specially ordered, leading to delays of several weeks.
This highlights the importance not only of clinician awareness, but also of public health preparedness. Healthcare systems should ensure that praziquantel remains accessible when cases are identified.
Further resources:
Unlimit Health: What is female genital schistosomiasis (FGS)?
More content in parasitic infections
Cite: touchINFECTIOUS DISEASES. 17 March 2026.
Editor: Katey Gabrysch, Editorial Director.
Disclosures: Dr Marc Steben has served on advisory boards for Merck and GSK and has participated in speaker bureau activities for both companies; and has received payments, honoraria or other forms of compensation from Bayer, Lupin, GSK, Roche Molecular Systems and Merck. Additional honoraria and grant support have been received from Abbott, BD/Waters, Attila/BioFire, Hologic, Laboratoire Médical Biron, Linepharma, Lupin, Merck/Merck Sharp & Dohme, Sanofi Pasteur, Paladin and Roche Molecular Systems.
Dr Marc Steben has also received honoraria from the non-governmental organisation HPV Global Action, of which he has served as co-president.
Dr Marc Steben owns Communications Action-Santé Inc. and Emotive Animation Studio and holds pharmaceutical investments through mutual funds.
Dr Marc Steben is currently participating in, or has participated within the past two years in, the Project PAVE clinical trial funded by the National Cancer Institute.
Dr Marc Steben has indicated that they do not hold any patents for products referred to in this educational activity or marketed by a commercial organization.
The content was developed and edited by human editors. No fees or funding were associated with its publication. touchINFECTIOUS DISEASES utilize AI as an editorial tool (ChatGPT (GPT-4o) [Large language model]. https://chat.openai.com/chat).
Images describing colposcopic findings associated with FGS have been reproduced with permission from: Female genital schistosomiasis: A pocket atlas for clinical health-care professionals. www.who.int/publications/i/item/9789241509299: World Health Organization; 2015. Licence: CC BY-NC-SA 3.0 IGO.
This content has been developed independently by Touch Medical Media for touchINFECTIOUS DISEASES in collaboration with Dr Marc Steben. Views expressed are the speaker’s own and do not necessarily reflect the views of Touch Medical Media.
SIGN UP to touchINFECTIOUS DISEASES!
Join our global community today for access to thousands of peer-reviewed articles, expert insights, and learn-on-the-go education across 150+ specialties, plus concise email updates and newsletters so you never miss out.

