This article provides an overview of nirmatrelvir/ritonavir (Paxlovid®; Pfizer, New York, NY, USA), an oral antiviral agent manufactured by Pfizer, used for treating mild-to-moderate coronavirus disease 2019 (COVID-19). Herein, we summarize the drug’s pharmacology, including its mechanism of action and pharmacokinetics, and review multiple clinical studies assessing its efficacy and safety across various patient populations, such as those with renal or hepatic impairment. Key findings indicate that nirmatrelvir/ritonavir is effective in reducing the progression of disease in high-risk, unvaccinated individuals, but studies show no significant benefit for post-acute COVID-19 symptoms or as a post-exposure prophylactic. Furthermore, it is critical to manage the numerous drug–drug interactions due to ritonavir’s enzyme-inhibitory properties and counsel patients on side effects such as dysgeusia and diarrhoea.
Following the outbreak of COVID-19, a myriad of treatment options were developed to combat COVID-19’s causative agent, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus. Remdesivir (Veklury®; Gilead Sciences Inc., Foster City, CA, USA ) was the first to receive Food and Drug Administration (FDA) approval.1,2 Remdesivir was developed by Gilead Sciences Inc. as an anti-Ebola agent and displayed efficacy against SARS-CoV-2. Immune modulators, such as baricitinib (Olumiant®; Eli Lilly, Indianapolis, IN, USA) and tocilizumab (Actemra®; Genentech Inc., San Francisco, CA, USA), were also repurposed for COVID-19 treatment. However, these formulations are used for patients with severe infection and primarily in the in-patient setting. For mild or moderate infections, oral agents that can be taken on an out-patient basis are desirable. Nirmatrelvir/ritonavir (Paxlovid™) was the first oral agent approved by the FDA for COVID-19 treatment. Molnupiravir (Lagevrio™; Merck Sharp & Dohme B.V., Haarlem, Netherlands) is currently the only other oral agent used for treatment that has an Emergency Use Authorization (EUA) from the FDA. Nirmatrelvir/ritonavir is a second-generation protease inhibitor that should be taken within 5 days of symptom onset. Herein, we will review the pharmacology and studies to date regarding nirmatrelvir/ritonavir’s efficacy and safety.
Pharmacology
Mechanism of action
The SARS-CoV-2 virus encodes two proteases, which are necessary for processing the pp1a and pp1ab polyproteins.3 Nirmatrelvir inhibits the SARS-CoV-2 main or 3C-like protease (Mpro/3CLpro), which blocks the polyprotein cleavage of functional proteins necessary for viral replication (Figure 1).4 Ritonavir is a pharmacokinetic enhancer, inhibiting the metabolism of nirmatrelvir via cytochrome P450 3A4 (CYP3A4) and subsequently increasing nirmatrelvir’s concentrations.
Figure 1: Transcription of SARS-CoV RNA
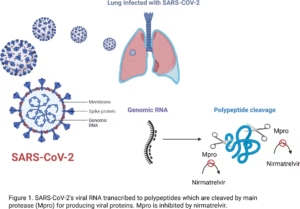
SARS-CoV-2’s viral RNA is transcribed into polypeptides, which are cleaved by main protease for producing viral proteins
Mpro is inhibited by nirmatrelvir.
Created with BioRender.com.
Mpro = main protease.
Pharmacokinetics
No dosage adjustments are required in patients with mild renal impairment (estimated glomerular filtration rate [eGFR] ≥60 to <90 mL/min). For patients with moderate renal impairment (eGFR ≥30 to <60 mL/min), 150 mg nirmatrelvir (one pill) + 100 mg ritonavir (one pill) should be used.5 In regard to patients with hepatic impairment, no dosage adjustment is needed in patients with mild (Child–Pugh Class A) or moderate (Child–Pugh Class B) hepatic impairment. No pharmacokinetic or safety data are available for patients with severe hepatic impairment (Child–Pugh Class C); thus, nirmatrelvir is not recommended for this patient population at the time of publication.
Administration of two 150 mg tablets of nirmatrelvir (with 100 mg of ritonavir) increased nirmatrelvir’s maximum plasma concentration (Cmax ) by approximately 60% and AUClast (area under the plasma concentration–time profile from time zero to time of the last quantifiable concentration) by 20% when administered with a high-fat meal compared with fasting. These increases in drug concentrations are not considered clinically relevant, and nirmatrelvir may be taken with or without food.6
Metabolism
Nirmatrelvir/ritonavir is contraindicated with drugs that are ‘highly dependent’ on CYP3A4 for clearance and with potent CYP3A inducers (e.g. rifampin, St John’s Wort).7,8
Formulation(s)
Currently, nirmatrelvir/ritonavir is available only as oral tablets co-packaged in a blister pack for 5 days.7,9 Lactose is included as an excipient; thus, patients with galactose intolerance or lactase deficiency should avoid using nirmatrelvir/ritonavir.
Study selection and data extraction
A literature search was conducted in PubMed and MEDLINE (from inception up to May 2025), using the search terms ‘Paxlovid’, ‘nirmatrelvir’, ‘COVID-19 treatment’ and ‘PF-07321332’. Approximately 6,357 results were identified for the search terms listed across both PubMed and MEDLINE. Studies currently being conducted were identified through ClinicalTrials.gov using the search terms ‘nirmatrelvir’, ‘paxlovid’ and ‘PF-07321332’, which yielded 22 results of completed, withdrawn and/or terminated studies. Reference lists of articles were also reviewed to identify any relevant articles, posters or conference abstracts. All relevant English-language studies, or studies that could be appropriately translated into English, containing results on the pharmacology, pharmacokinetics, safety and efficacy of nirmatrelvir/ritonavir were selected for review and are included in this article. Studies that did not have results were ongoing or were unrelated to the topics discussed were excluded.
In vitro studies
The in vitro efficacy of nirmatrelvir, the active component of Paxlovid, against the SARS-CoV-2 Mpro variants associated with Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), Lambda (B.1.1.1.37/C37) and Omicron (B.1.1.529) was evaluated by Greasley et al.10 Kinetic analyses showed that key mutations in Mpro (K90R, G15S and P132H) did not significantly alter catalytic efficiency (kcat/Km) compared with the wild-type protease. Inhibition assays confirmed that nirmatrelvir retained potent inhibitory activity across all variants, with inhibition constants (Ki) ranging from 0.64 nM for the Omicron variant to 4.07 nM for the Lambda variant, and 0.93 nM for the wild-type enzyme. Structural studies, including high-resolution crystallography (1.63–2.09 Å) and hydrogen–deuterium exchange mass spectrometry, demonstrated that these mutations are distal to the nirmatrelvir-binding site and do not disrupt the structural integrity of the binding pocket or nirmatrelvir’s binding mode. These findings support the continued effectiveness of nirmatrelvir against evolving SARS-CoV-2 variants and its role in combating COVID-19.10
Kong et al. identified a potential side effect of nirmatrelvir/ritonavir, a COVID-19 antiviral, by investigating its effects on chondrocytes in vitro.11 Nirmatrelvir/ritonavir inhibited extracellular matrix protein secretion, including collagen and proteoglycans, in a dose-dependent manner and downregulated the chondrogenic markers SRY-box transcription factor 9 (Sox9) and collagen type II alpha 1 chain (Col2a1). Mechanistically, nirmatrelvir/ritonavir induced endoplasmic reticulum (ER) stress through activation of the inositol-reequiring enzyme 1 alpha (Ire1α)–x-box protein binding 1 (Xbp1s), protein kinase R (PKR)-like endoplasmic reticulum kinase (PERK)–eukaryotic initiation factor 2a (eIF2α)–activating transcription factor 4 (Atf4) and activating transciption factor 6 (Atf6) pathways, and disrupted redox homeostasis, increasing reactive oxygen species (ROS) levels and ferroptosis. Rescue experiments with ER stress and ROS inhibitors partially restored matrix secretion and reduced cellular stress. These findings suggest that while nirmatrelvir/ritonavir is crucial for COVID-19 treatment, its potential to accelerate chondrocyte senescence and cartilage degeneration warrants further investigation.11
Jochmans et al. explored the potential for SARS-CoV-2 to develop resistance to 3C-like protease (3CLpro) inhibitors, including nirmatrelvir, through serial passaging in vitro.12 The study identified a triple substitution in the 3CLpro enzyme that significantly increased resistance, with half-maximal effective concentration (EC50) values rising up to 72-fold for nirmatrelvir and 93-fold for ensitrelvir compared with the wild-type enzyme. Individual substitutions (E166A and L167F) showed low-level resistance, but the triple mutation exhibited the highest resistance and cross-resistance to multiple inhibitors. Structural analysis revealed that these mutations reduced inhibitor–enzyme interactions, particularly by disrupting hydrogen bonds and altering binding pocket dynamics, while maintaining sufficient substrate binding to sustain enzymatic activity. Despite these resistance-associated changes, the triple-mutant virus retained full susceptibility to the polymerase inhibitor remdesivir, suggesting specificity in resistance mechanisms. These findings emphasize the importance of monitoring resistance development in 3CLpro-targeting therapeutics such as nirmatrelvir/ritonavir and highlight the need for combination antiviral strategies to mitigate resistance risks.12
Clinical studies
A search for completed studies on ClinicalTrials.gov yielded 27 results using the search string ‘Other terms: COVID-19 treatment | paxlovid OR nirmatrelvir OR PF-07321332’. Studies describing nirmatrelvir/ritonavir, or the aforementioned drugs, in the setting of COVID-19 treatment were included, while studies exploring the primary properties of the drug, phase I studies, observational studies, studies without published results or those with a withdrawn or unknown status were excluded from this section of the review (Table 1).13–21
Table 1: Findings from nirmatrelvir/ritonavir clinical studies13–21
| Trial/study reference | Study type | Study population | Primary outcome(s) | Key findings |
| Safety and clinical and virological outcomes in patients with CKD treated with nirmatrelvir/ritonavir (NCT05624840)13 | Observational, prospective, single-arm | 85 adults with advanced CKD (eGFR <30 mL/min/1.73 m²) infected with COVID-19 | AEs | AEs in 9.4% and SAEs in 5.9%. Significant viral-load reduction at days 5, 15 and 30 (p<0.001); 97% achieved viral clearance by day 30. 10 patients experienced transient, asymptomatic rebound |
| Renal impairment study of PF-07321332 boosted with ritonavir (NCT04909853)14,15 | Phase I, nonrandomized, open-label | 30 adults aged 18–75 years with normal, mild, moderate or severe renal impairment | Pharmacokinetics (Cmax, AUCinf, Ae48, renal clearance) | Systemic exposure to nirmatrelvir increased with renal impairment (AUC 123.8%, 187.4% and 304.5% for mild, moderate and severe, respectively). Cmax 129.8%, 138.1% and 148.0%, respectively. Apparent clearance decreased with lower eGFR. Mild AEs across groups; one SAE led to discontinuation in severe impairment |
| Nirmatrelvir/ritonavir in participants with hepatic impairment (Singh et al.)16 | Phase I, nonrandomized, open-label | 16 adults: 8 with moderate hepatic impairment, 8 with normal liver function | Pharmacokinetics (Cmax, AUClast, AUCinf) | Nirmatrelvir AUC and Cmax comparable between groups; AEs in 3/8 normal versus 4/8 impaired; no significant lab or ECG changes |
| STOP-PASC Clinical Study (Geng et al.)17 | Phase II, double-blind, placebo-controlled RCT | 155 adults with moderate-to-severe PASC symptoms ≥3 months post-COVID-19 | Pooled severity of six PASC symptoms (fatigue, brain fog, SOB, body aches, GI and CV) at 10 weeks | No significant difference versus placebo in symptom severity or functional outcomes; AEs common (nirmatrelvir/ritonavir: 99%), mostly mild |
| EPIC-HR (Hammond et al., 2022; NCT04960202)18 | Phase II/III, randomized, double-blind, two-arm | 2,246 unvaccinated, high-risk adults with mild–moderate COVID-19, symptom onset ≤5 days | Percentage of COVID-19-related hospitalization or death over 28 days | Hospitalization/death: 6.3% reduction compared with placebo, p<0.001; 0 deaths in treatment versus 13 in placebo. Viral load lower at day 5 with treatment. AEs: dysgeusia (5.6%) and diarrhoea (3.1%) more frequent with nirmatrelvir/ritonavir; overall AE rates similar between groups |
| EPIC-PEP (Hammond et al., 2023; NCT05047601)19 | Phase II/III, randomized, double-blind, double-dummy, placebo-controlled | 2,736 adults exposed to SARS-CoV-2 within 4 days in the same household (no current infection) | Development of symptomatic, confirmed COVID-19 through day 14 | Symptomatic infection: 5-day Paxlovid = 29.8% risk reduction versus placebo (p=0.17); 10-day = 35.5% (p=0.12); differences not significant. AEs: comparable across groups; no new safety signals |
| Modern directed antiviral COVID-19 therapy (Balykova et al., 2022)20 | Open-label, two-stage, multicentre | Stage I: healthy volunteers; stage II: 264 adults (18–80 years) with mild–moderate COVID-19 (132 combination, 132 standard therapy) | Efficacy (recovery rate, RNA negativity); safety | No progression to severe disease in treatment versus some in control; complete recovery day 6: 35.6% treatment versus ≈18% control (p=0.0001); RNA negativity: 82.6% versus ≈62% (p=0.0001); AEs transient, no discontinuations |
| Haemodialysis study (Lu et al., 2023)21 | Phase IV, prospective, two-step, nonrandomized, open-label | 41 adults (35 on haemodialysis, 6 had normal renal function); compared 150 or 300 mg nirmatrelvir + 100 mg ritonavir BID for 5 days | Pharmacokinetics (Cmin); safety (AEs, drug-related AEs); virological clearance | AEs in 3 (step 1, 150 mg) and 7 (step 2, 300 mg) participants (p=0.025); drug-related AEs in 2 and 6 participants, respectively (p=0.054); Cmin (ng/mL): 5,295 ± 2371 (step 1), 7,676 ± 2745 (step 2), versus 2,274 ± 1,347 (control); no difference in viral clearance (p=0.232); no SAE or hepatic toxicity observed |
AE = adverse event; Ae48 = Amount excreted unchanged in urine over 48 h; AUC = area under the curve; AUCinf = area under the plasma concentration-time profile from time zero (0) to extrapolated infinite time; AUClast = area under the plasma concentration–time profile from time zero to time of the last quantifiable concentration; BID = twice daily; CKD = chronic kidney disease; Cmax = maximum plasma concentration; Cmin = minimum plasma concentration; COVID-19 = coronavirus disease 2019; CV = cardiovascular symptom; ECG = electrocardiogram; eGFR = estimated glomerular filtration rate; GI = gastrointestinal symptom; PASC = post-acute sequelae of SARS-CoV-2 infection; RCT = randomized clinical trial; SAE = serious adverse event; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; SOB = shortness of breath.
A prospective, single-arm interventional study evaluated the safety, clinical and virological outcomes of a modified dose of nirmatrelvir/ritonavir in patients with advanced chronic kidney disease (CKD) who were infected with COVID-19.13 The study recruited 85 adult patients with CKD, of whom 59 (69.4%) were on dialysis and had an eGFR of <30 mL/min/1.73 m². The primary outcomes assessed were the safety profile, including adverse events (AEs) and serious adverse events (SAEs), and the clinical and virological outcomes, such as changes in viral load measured by polymerase chain reaction (PCR) and rapid antigen tests, and any signs of virological or symptomatic rebound. Of the 85 participants, 80 (94.1%) completed the full treatment course. AEs were reported in 9.4% of patients, while SAEs occurred in 5.9% of the cohort; these rates were comparable between those with eGFR values of <30 and ≥30 mL/min/1.73 m². The viral load showed a significant reduction on days 5, 15 and 30 post-treatment initiation (p<0.001 for all time points). Ten patients experienced virological rebound, which was transient and asymptomatic. Cough and fatigue were the most frequent symptoms during treatment, resolving on average within 18.3 days, with no significant difference between patients with low and high eGFRs (p=0.7). By day 30, all patients were asymptomatic, and the PCR results showed a high rate of viral clearance at 43.7 ± 4.0 (p<0.001), and 97.2% of participants had cycle threshold (Ct) values above 30. The study demonstrated that a modified dose of nirmatrelvir/ritonavir is generally well tolerated and effective in reducing viral load in patients with advanced CKD, including those on dialysis. Although there were instances of virological rebound, they were mostly asymptomatic and did not lead to severe clinical outcomes. These findings suggest that nirmatrelvir/ritonavir can be safely considered for use in this high-risk patient population, with appropriate dose adjustments based on renal function.13
In a phase I, nonrandomized, open-label study, Toussi et al. investigated nirmatrelvir/ritonavir in the setting of renal impairment.14 Participants aged 18–75 years included those with normal-to-severe renal impairment and received a 100 mg dose of ritonavir administered 12 h before, during and after a 100 mg dose of nirmatrelvir. To meet inclusion criteria, participants with impaired renal function must not have other significant comorbidities. Individuals with hepatitis B or C, those who were pregnant or breastfeeding and those with other possible confounding factors were excluded. The results demonstrated that systemic exposure to nirmatrelvir was directly correlated with the severity of renal impairment. Compared with participants who had normal renal function, the adjusted geometric mean area under the curve (AUC) values were 123.8%, 187.4% and 304.5% for participants with mild, moderate and severe renal impairment, respectively. Corresponding Cmax values were 129.8%, 138.1% and 148.0%. Similarly, apparent clearance was directly correlated with higher eGFR, with reductions of ~47% and 80% in participants with moderate and severe renal impairment, respectively. Despite these changes in exposure, nirmatrelvir/ritonavir was generally well tolerated across all groups, with mild treatment-related AEs. One patient in the severe renal impairment group did not complete the study due to a serious AE on day 2. Based on these findings, the authors concluded that a dose reduction to 150/100 mg nirmatrelvir/ritonavir twice daily is recommended for patients with moderate renal impairment, while no dosage adjustment is needed for those with mild renal impairment. However, for those with severe renal impairment, nirmatrelvir is not currently recommended. This study provides important insights into adjusting treatment regimens for patients with SARS-CoV-2 infection and renal impairment to ensure both efficacy and safety.14,15
Singh et al. conducted a phase I, nonrandomized, open-label study to assess the pharmacokinetics and safety of nirmatrelvir/ritonavir in individuals with hepatic impairment.16 The study included 16 participants: eight with moderate hepatic impairment and eight with normal liver function. Each participant received a single 100 mg dose of nirmatrelvir alongside 100 mg of ritonavir, administered at specified intervals before, during and after nirmatrelvir dosing. The findings indicated that the median plasma concentrations and overall exposure to nirmatrelvir, assessed by AUC and Cmax, were similar between both groups. While three of eight participants in the normal hepatic function group had a treatment–emergent AE, compared with four in the moderate impairment group, the safety of the nirmatrelvir/ritonavir combination was found to be satisfactory across all participants, with no significant changes observed in laboratory values, vital signs or electrocardiogram results. Median plasma concentrations at 48 h were also similar. These results suggest that dose adjustments for nirmatrelvir/ritonavir are not required for patients with moderate hepatic impairment, and potentially not for those with mild impairment either. This study offers important insights into the safe administration of nirmatrelvir/ritonavir in patients infected with SARS-CoV-2 and different levels of liver function.16
The Selective Trial of Paxlovid for PASC (STOP-PASC) Randomized Clinical study, reported by Geng et al., assessed the efficacy of a 15-day course of nirmatrelvir/ritonavir in alleviating symptoms of post-acute sequelae of SARS-CoV-2 infection (PASC).17 This double-blind, placebo-controlled study included 155 participants, all with moderate-to-severe PASC symptoms lasting 3 months or longer. Participants were randomly assigned to receive either nirmatrelvir/ritonavir (300 and 100 mg) or a placebo with ritonavir. The primary outcome was the severity of six PASC symptoms – fatigue, brain fog, shortness of breath, body aches, gastrointestinal issues and cardiovascular symptoms – evaluated 10 weeks after treatment initiation. Study findings revealed no significant difference between the treatment and placebo groups in reducing the severity of PASC symptoms at 10 weeks. Secondary outcomes, including patient-reported measures and physical function tests, also showed no substantial benefits of nirmatrelvir/ritonavir over placebo. The most common symptoms reported by participants were fatigue (45.2%) and brain fog (24.5%). Most participants experienced AEs across both treatment groups; 99% of those in the treatment group reported an AE compared with 92.5% in the placebo group, most of which were low grade. Despite being generally safe, the treatment did not provide significant relief for PASC symptoms in this mostly vaccinated cohort with prolonged symptoms.
In a phase II/III study, Hammond et al. evaluated the effect of nirmatrelvir plus 100 mg of ritonavir versus placebo on hospital admission and death rates in unvaccinated, high-risk symptomatic individuals with SARS-CoV-2.18 Participants were required to have a coexisting condition or trait that deemed them at high risk for disease progression, such as body mass index (BMI) greater than 25, current smoking status or hypertension, to meet inclusion criteria. Those who had a previous infection with SARS-CoV-2 or COVID-related hospitalization, anticipated hospitalization, symptom onset greater than 5 days prior to randomization or recipients of convalescent SARS-CoV-2 plasma or SARS-CoV-2 vaccinations were not eligible. Participants were assigned in a 1:1 ratio to treatment or placebo and received 10 doses, 12 h apart, over a course of 5 days. Participants were evaluated for 28 days for hospitalization or death, and 1,717 of 3,000 patients enrolled were statistically assessed for safety, efficacy and viral load. With regard to efficacy, results suggested a positive role in reducing progression of disease in the high-risk population. In a modified intention-to-treat analysis evaluating those who received treatment within 3 days of symptom onset, there was a 6.32% reduction in hospitalization rate compared with placebo (p<0.001). The incidence and death rates were also lower in the treatment group, with 0.77% and zero deaths versus 7.01% and seven deaths, respectively. All deaths occurred in the placebo group. Additionally, viral load was lower at day 5 of treatment in the nirmatrelvir/ritonavir group, but AEs were similar in both study arms. Participants in the treatment group also experienced more dysgeusia (5.6% versus 0.3%) and diarrhoea (3.1% versus 1.6%) than those receiving placebo.18
Hammond et al. also examined the role of nirmatrelvir/ritonavir in SARS-CoV-2 for prophylaxis.19 The phase II/III, randomized, double-blind, double-dummy, placebo–controlled study narrowed focus on individuals who had been exposed to COVID-19 in their household within the last 4 days but did not yield a positive test result for current infection. Those with a history of COVID-19 infection within the 6 months prior to the study, or high-risk individuals, such as those with high fever, CKD, pregnancy or breastfeeding, HIV with a high viral load or previous COVID-19 treatment within 6 months, were excluded. The study followed a 10-day treatment plan, where participants were randomized in a 1:1:1 ratio to receive either placebo only (898 participants), PF-07321332/ritonavir only (917 participants) or PF-07321332/ritonavir for days 1–5 and then placebo for days 6–10 (921 participants). Treatments were given 12 h apart throughout the treatment period. Progression to symptomatic or confirmed infection with COVID-19, as well as other factors such as emergent AEs, symptoms and viral load, was assessed at various time points following treatment. Results suggest that nirmatrelvir/ritonavir may not be effective prophylactically in this setting, as test-positive, symptomatic SARS-CoV-2 infection rates were similar across all groups, with treatment:placebo risk reductions being 29.8% for the 5-day treatment group (p=0.17) and 35.5% for the 10-day treatment group (p=0.12). Similarly, there was no significant difference among participants considered high risk for progression of disease or AE rates.19
An open-label, two-stage, multicentre study evaluated the efficacy and safety of a fixed combination of nirmatrelvir 300 mg and ritonavir 100 mg in patients with COVID-19.20 In the first stage, safety and pharmacokinetic parameters were assessed in healthy volunteers. The second stage involved 264 patients with COVID-19 aged 18–80 years, with 132 patients receiving the combination therapy and 132 receiving standard therapy. The results showed that none of the patients in the nirmatrelvir and ritonavir groups experienced progression to severe disease, unlike those in the standard therapy group. By day 6, 35.61% of patients in the combination therapy group achieved complete recovery – double that of the standard therapy group (p=0.0001). Additionally, 82% of patients in the combination therapy group tested negative for SARS-CoV-2 RNA, 20% higher than in the standard therapy group (p=0.0001). The combination therapy was well tolerated, with transient adverse reactions not requiring discontinuation or modification of treatment. This study highlights the potential of the fixed combination of nirmatrelvir and ritonavir as a superior alternative to standard COVID-19 therapy, offering a favourable safety profile and significantly improved recovery rates. The findings support the clinical and pharmacoeconomic feasibility of incorporating this combination into COVID-19 treatment protocols, particularly in preventing disease progression and enhancing patient recovery outcomes.20
In the prospective, two-step, nonrandomized, open-label, phase IV study, Lu et al. aimed to fill the gap in data regarding the use of nirmatrelvir/ritonavir in patients undergoing haemodialysis.21 To evaluate safety and the rate of AEs, researchers administered a 5-day regimen of either 150 mg nirmatrelvir once daily with 100 mg ritonavir twice daily, or 300 mg nirmatrelvir once daily with 100 mg ritonavir twice daily. The study included six patients with normal renal function and compared them with 35 patients undergoing haemodialysis. Among the patients receiving 150 mg of nirmatrelvir, three out of 10 experienced AEs, while seven out of eight in the 300 mg group reported AEs (p=0.025). Notably, two out of three in the 150 mg group and six out of seven in the 300 mg group had drug-related AEs (p=0.054), indicating that both doses were excessively high for the haemodialysis population. Additionally, there was no significant difference in viral elimination time between those who received nirmatrelvir and those who did not (p=0.232). These findings underscore the conclusion that this treatment may not be suitable for all patient populations.21
Other notable reports
Because our original search captures only interventional trials, we conducted a supplementary manual search of peer-reviewed journals and major medical news outlets to identify post-marketing or observational reports on nirmatrelvir/ritonavir. These were included narratively to provide a complete perspective on emerging evidence. Three studies were identified.
A population-based natural experiment from Ontario, Canada, evaluated whether expanded access to nirmatrelvir/ritonavir reduced hospitalization or mortality among 1,620,884 vaccinated adults aged 65–74 years.22 During a policy period restricting access to those aged ≥70 years, prescription rates more than doubled above this threshold (115% increase), but no significant differences were observed in COVID-19-related hospitalizations (39.5 versus 42.9 per 100,000 per month; p=0.15), all-cause hospitalizations (979.6 versus 988.4; p=0.69) or all-cause mortality (109.6 versus 115.7; p=0.17). The estimated treatment effect corresponded to a nonsignificant 2.8-percentage-point increase in hospitalization risk (95% confidence interval: -1.3 to 6.9). These findings suggest that, in a highly vaccinated older population, expanded access to nirmatrelvir/ritonavir did not translate into measurable reductions in severe outcomes. A JAMA (Journal of the American Medical Association) Medical News & Perspectives piece described ‘COVID-19 rebound’ after nirmatrelvir/ritonavir, highlighting case reports of symptom and test positivity recurrence days after initial recovery and negative tests; the Centers for Disease Control and Prevention’s (CDC’s) May 24 Health Alert characterized such rebounds as typically mild and self-limited (≈3 days), while continuing to recommend treatment for eligible patients.23 The authors noted that the mechanism remained uncertain: FDA and CDC note that rebounds may occur as part of the SARS-CoV-2’s natural history (EPIC-HR [Evaluation of Protease Inhibition for Covid-19 in High-Risk Patients] reanalysis found ~1–2% post-negative positives in both active and placebo arms), whereas other reports posit timing or duration effects. Limited observational data were noted to suggest possible transmission during relapse in household settings.
A narrative review summarized randomized evidence on nirmatrelvir/ritonavir for acute COVID-19.24 Two Pfizer-sponsored randomized clinical trials (RCTs) were identified: AN INTERVENTIONAL EFFICACY AND SAFETY, PHASE 2/3, DOUBLE-BLIND, 2 ARM STUDY TO INVESTIGATE ORALLY ADMINISTERED PF 07321332/RITONAVIR COMPARED WITH PLACEBO IN NONHOSPITALIZED SYMPTOMATIC ADULT PARTICIPANTS WITH COVID-19 WHO ARE AT LOW RISK OF PROGRESSING TO SEVERE ILLNESS (ClinicalTrials.gov identifier: NCT05011513) and AN INTERVENTIONAL EFFICACY AND SAFETY, PHASE 2/3, DOUBLE-BLIND, 2-ARM STUDY TO INVESTIGATE ORALLY ADMINISTERED PF-07321332/RITONAVIR COMPARED WITH PLACEBO IN NONHOSPITALIZED SYMPTOMATIC ADULT PARTICIPANTS WITH COVID-19 WHO ARE AT INCREASED RISK OF PROGRESSING TO SEVERE ILLNESS (ClinicalTrials.gov identifier: NCT04960202).18,25 The first, EPIC-HR, enrolled 2,246 unvaccinated high-risk out-patients and found a reduction in hospitalization or death (6.3% placebo versus 0.8% nirmatrelvir/ritonavir; p<0.001). The unpublished EPIC-SR trial included 1,288 lower risk, largely vaccinated or previously infected adults and showed no difference between groups (0.8% versus 1.6%; p=0.2), leading to early termination.24 The authors emphasized that EPIC-HR’s unvaccinated cohort limits its relevance to current populations and that the unpublished EPIC-SR trial better reflects present-day conditions. A prospective study cited found virologic rebound in 21% of nirmatrelvir/ritonavir recipients versus 2% of controls (number needed to harm=5), raising questions about incomplete viral clearance. Overall, the review concluded that, aside from EPIC-HR, no published trial demonstrates clinical benefit, and it highlighted concerns regarding ritonavir-related drug interactions, incomplete publication of negative trials and uncertain generalizability of existing evidence.24
Safety and adverse effects
The two most commonly reported side effects (with a ≥1% incidence) were dysgeusia and diarrhoea.5,6 The dysgeusia reported with nirmatrelvir/ritonavir is sometimes referred to as ‘Paxlovid Mouth’.26 According to the manufacturer, 5% of patients will experience dysgeusia. Other side effects have been reported but are considered rare. These include abdominal pain, hypertension, headache and malaise; additionally, cases of Stevens–Johnson syndrome, toxic epidermal necrolysis and other hypersensitivity reactions have been reported.5,27
Pregnancy/lactation
No difference in the rate of overall birth defects among live births following exposure to ritonavir has been observed compared with the background birth defect rate.5,6 To date, little is known about the effects of nirmatrelvir on humans. Lower birth weight was reported in rabbits with 10 times the clinical exposure as authorized human doses; thus, the use of nirmatrelvir/ritonavir is not recommended in pregnant women.
Relevance to patient care
Drug–drug interactions are numerous with nirmatrelvir/ritonavir, primarily due to ritonavir’s strong CYP3A4-inhibitory properties (Table 2).5,7,28,29 With regard to CYP3A4 inhibition, treatment may require one of the following: an alternative COVID-19 medication (e.g. patient taking amiodarone), an alternative interacting medication (e.g. clopidogrel to prasugrel), withholding treatment for a period of time (e.g. statins) or simply managing the interaction if considered ‘minor’. Ritonavir has also been shown to inhibit CYP2D6 (cytochrome P450)2D6 and drug transporters such as MDR1 (multi-drug resistance 1) and OATPB1 (organic anion-transporting polypeptide 1B1). Of note, however, not all drug–drug interactions with ritonavir are inhibitory; ritonavir is an inducer of the following enzymes: CYP1A2, CYP2B6, CYP2C8, CYP2C9 and CYP2C19. Substrates of these enzymes may have reduced concentrations when taken concomitantly with nirmatrelvir/ritonavir. As nirmatrelvir is a substrate of CYP3A4, drug inducers may decrease its concentrations; potent enzyme inducers are contraindicated (e.g. carbamazepine, phenytoin).
Table 2: Commonly used drugs, their mechanism of interaction with nirmatrelvir/ritonavir and recommended actions to be taken5,7,28
| Therapeutic drug class | Specific drug | Drug–drug interaction | Recommendation |
| HMG Co-A reductase inhibitors (statins) | Lovastatin, simvastatin | Highly dependent on CYP3A metabolism. Inhibition leads to increased plasma concentrations, risking myopathies, including rhabdomyolysis | Contraindicated. Do not co-administer. Discontinue these statins at least 12 h prior to nirmatrelvir/ritonavir and hold for at least 3 days (preferably 5 days) after nirmatrelvir/ritonavir completion |
|
| Atorvastatin, rosuvastatin, fluvastatin, pravastatin | Less dependent on CYP3A or not dependent, but exposure may still increase (rosuvastatin AUC increased 31%, Cmax 112%) | Administer the lowest possible dose of atorvastatin or rosuvastatin. Consider temporary discontinuation of fluvastatin and pravastatin during nirmatrelvir/ritonavir treatment |
| Anticonvulsants (CYP3A inducers) | Carbamazepine, phenobarbital, phenytoin, primidone | Strong CYP3A4 inducers. Decreases nirmatrelvir/ritonavir exposure (carbamazepine decreased nirmatrelvir AUC by 55%), risking loss of virologic response and resistance. Induction persists after drug cessation | Contraindicated. Do not co-administer. Alternative COVID-19 therapy recommended |
| Sedatives/hypnotics | Oral midazolam, triazolam | Highly dependent on CYP3A4 metabolism (oral midazolam AUC increased 1,330%). Risks extreme sedation and respiratory depression | Contraindicated Pause the anxiolytic during, and for at least 3 days (up to 5 days), after nirmatrelvir/ritonavir completion |
| Antiarrhythmics | Dronedarone, propafenone, quinidine | Increased plasma concentrations risk arrhythmias and serious adverse events | Contraindicated |
|
| Amiodarone | Has a very long elimination half-life (approximately 55 days). Increased exposure risk cannot be mitigated by short-term pausing | Contraindicated. Do not co-administer. Alternative COVID-19 therapy is recommended |
| Calcineurin/mTOR inhibitors (immunosuppressants) | Tacrolimus, cyclosporine, everolimus, sirolimus | Narrow therapeutic index drugs dependent on CYP3A4/P-gp metabolism. Ritonavir profoundly increases exposure, risking toxicity (e.g. neurotoxicity, nephrotoxicity, acute kidney injury) | Alternative COVID-19 treatment should be considered as management is complex and requires TDM, which may not be feasible outside a clinical setting |
| Oral anticoagulants (DOACs) | Rivaroxaban | Inhibition of CYP3A and P-gp leads to increased plasma levels (AUC increased 153%) and risk of bleeding | Avoid concomitant use/not recommended Requires pausing the drug and using alternative anticoagulation (e.g. LMWH) if indicated, or switching to an alternative DOAC that is dose-adjusted (apixaban) |
|
| Apixaban | Combined CYP3A4 and P-gp inhibition increases blood levels | Reduce dose by 50% (for 5 or 10 mg dose) or avoid (if already taking 2.5 mg BID) |
|
| Dabigatran | P-gp substrate; AUC increased twofold | Reduce dose (110 mg twice daily for normal renal function; 75 mg twice daily for moderate renal impairment) |
|
| Warfarin | Metabolism by multiple CYPs (CYP2C9/3A4/1A2). Ritonavir inhibits CYP3A4 (increasing exposure) while inducing CYP1A2/2C9 (decreasing exposure). An increase in warfarin exposure is anticipated with a short nirmatrelvir/ritonavir course | Monitor INR as clinically indicated |
| Antiplatelets | Clopidogrel | Nirmatrelvir/ritonavir may reduce conversion to clopidogrel’s active metabolite (metabolized by CYP3A4/2C19/2B6/1A2), leading to insufficient platelet inhibition. This is risky after coronary stenting | Avoid in patients at very high risk of thrombosis (e.g. early period post coronary stenting). If feasible, temporarily substitute with prasugrel. May be considered if transient loss of efficacy is acceptable |
| Opioid analgesics | Oxycodone, fentanyl | Metabolized extensively by CYP3A4. Ritonavir increases plasma concentrations (oxycodone AUC increases threefold). Risks of opioid toxicity, including respiratory depression | Consider dosage reduction and closely monitor for therapeutic and adverse effects (e.g. respiratory depression) |
| Calcium channel blockers | Amlodipine, diltiazem, felodipine, nicardipine, nifedipine, verapamil | Primarily metabolized by CYP3A4. Ritonavir increases concentrations (amlodipine AUC increased twofold) | Monitor/dose adjustment. Amlodipine dose reduction by 50% is generally recommended/optional |
| Respiratory agents | Salmeterol | CYP3A4 substrate. Pronounced increase in plasma concentrations risks serious and/or life-threatening cardiovascular adverse events (e.g. QT prolongation) | Avoid concomitant use |
| Antipsychotics | Quetiapine | CYP3A4 substrate. Expected up to an eightfold increase in AUC. Risks QT interval prolongation and destabilization | Contraindicated (per some labels). If used, management is challenging: consult a specialist for dose reduction and close monitoring |
| Steroids (corticosteroids) | Budesonide, fluticasone, triamcinolone, dexamethasone | CYP3A4 substrates. Increased exposure risks systemic corticosteroid effects, such as Cushing’s syndrome and adrenal suppression, especially with high-dose/long-term ritonavir | Caution/monitoring. Risk is low due to a short course. Monitoring for systemic side effects is recommended, especially for long half-life steroids like triamcinolone. Consider dose reduction or switching to a non-CYP3A4 substrate corticosteroid |
| Hormonal contraceptives | Ethinyl estradiol (combined oral contraceptives) | Ritonavir may induce CYP1A2 and UGT (via induction, not fully established during short course). Ritonavir is likely to reduce the efficacy of estradiol-containing contraceptives | Advise patients to use an effective alternative or additional barrier method of contraception during treatment with nirmatrelvir/ritonavir, and until one menstrual cycle after stopping nirmatrelvir/ritonavir |
| DPP4 inhibitors (antidiabetics) | Saxagliptin | Primarily metabolized by CYP3A4; AUC substantially increased by strong inhibitors. Risks of hypoglycaemia | Dose adjustment. Saxagliptin dose should not exceed 2.5 mg once daily |
| Migraine products | Eletriptan | Co-administration within 72 h of nirmatrelvir/ritonavir is contraindicated due to potential for serious adverse reactions, including cardiovascular and cerebrovascular events | Contraindicated |
| Anti-gout | Colchicine | CYP3A4 and P-gp inhibition leads to increased concentrations. Life-threatening and fatal drug interactions have been reported | Contraindicated |
AUC = area under the curve; BID = twice daily; COVID-19 = coronavirus disease 2019; CYP = cytochrome p450 enzymes; CYP3A = cytochrome 3A; CYP3A4 = cytochrome 3A4; DOAC = direct oral anticoagulant; DPP-4 = dipeptidyl peptidase-4; HMG-Co-A = 3-hydroxy-3-methylglutaryl-coenzyme A; INR = International Normalized Ratio; LMWH = low molecular weight heparin; mTOR = mammalian target of rapamycin; P-gp = p-gylcoprotein; TDM = therapeutic drug monitoring; UGT = UDP-glucuronosyltransferase.
In addition to multiple drug–drug interactions, viral rebound has been observed with nirmatrelvir/ritonavir use.30–32 It is believed that nirmatrelvir/ritonavir inhibits viral growth but may not fully clear the virus; therefore, if immune function is not fully restored, then a rebound in virus may occur once nirmatrelvir/ritonavir treatment is completed.33
Beyond clinical considerations, the economic implications of nirmatrelvir/ritonavir use warrant discussion. At the time of this publication, nirmatrelvir/ritonavir remains a high-cost antiviral, with initial US commercial pricing estimated at approximately $1,400 per treatment course following transition from government purchase to private distribution, thereby posing accessibility barriers.34 Broader access will require coordinated international efforts to expand generic licensing, reduce manufacturing costs and implement tiered or subsidized pricing models.
Advantages and limitations of this article
This article offers a comprehensive evaluation of the pharmacology, safety and efficacy of nirmatrelvir/ritonavir, integrating findings from clinical, pharmacokinetic and post-marketing studies. Strengths include a structured search of ClinicalTrials.gov, ensuring the capture of all completed interventional trials with available results, and the inclusion of detailed pharmacologic data to contextualize clinical outcomes. In addition, a supplemental search identified peer-reviewed letters, narrative reviews and research news articles describing neutral or negative findings, thereby providing a balanced appraisal that extends beyond the limitations of formal trial registries.
Several limitations should be acknowledged. This article did not employ a formal systematic methodology and was restricted to English-language publications, potentially introducing selection bias. Some pivotal studies, including Pfizer-sponsored trials such as EPIC-SR, remain unpublished or incompletely reported, which limits a comprehensive assessment of the total evidence base. Furthermore, variations in study design, population characteristics (notably vaccination status and circulating variants) and endpoints complicate direct comparisons and may affect generalizability to current clinical practice. Finally, inclusion of narrative and media-based reports, while valuable for completeness, represents secondary sources rather than primary empirical data. Despite these constraints, this article synthesizes the most current and relevant information available, providing an objective overview of nirmatrelvir/ritonavir’s evolving role in the management of COVID-19.
Conclusion
In addition to molnupiravir, nirmatrelvir/ritonavir provides an oral option for COVID-19 treatment, which reduces both mortality and hospitalization.35–37 Drug–drug interactions limit nirmatrelvir/ritonavir use in specific cases, requiring the cessation or adjustment of medications at times. Additionally, a small percentage of patients will experience AEs that lead to nonadherence. Overall, nirmatrelvir/ritonavir provides a useful medication for patients with mild-to-moderate COVID-19 symptoms but may have limited efficacy in vulnerable populations (e.g. elderly). Though drug–drug interactions and adverse effects potentially complicate treatment, a 5-day duration limits sustained monitoring and long-term modification of concomitant medications. There is also a need for further studies to address long-term safety, resistance development and efficacy as it relates to future COVID-19 variants.